|
|
Post by duwayne on Jun 5, 2021 16:49:24 GMT
I find the headline “Previous Infection is Superior to Vaccine for COVID Protection” may be a bit of a stretch, even based on the article itself. The article says in an early paragraph “We need to get vaccinated because vaccines are highly efficacious. They are better than the traditional response you get from natural infection.” (This is a quote from Fauci referencing 3 recent studies.) The article says later “…an Israeli study with over 6 million participants directly compared the risk of infection (or reinfection) of people who had been vaccinated with that of people who had not been vaccinated but who had survived a COVID infection. They found that the risk of infection for both groups was equivalent…” Here's another article which says that infection doesn’t provide close to full immunity from reinfection. “Although most people infected with COVID-19 have about 80% immunity from catching it again for at least six months, people age 65 and older have less than 50% immunity, the data showed.” www.upi.com/Health_News/2021/03/17/coronavirus-reinfection-study/8961616008058/It would seem that you are pretty much immune from future serious outcomes (death or long-lasting health disorders) from either a vaccination or past infection. That does not rule out the possibility that one might be a little better than the other for your particular situation (age, race, natural immunity, etc) or for some particular variant or future mutation. The article also contains this statement… “As of May 21, the CDC’s own Vaccine Adverse Event Reporting System (VAERS) lists 262,521 reports of adverse events. Here are some of the events associated with COVID vaccination included in these reports: 4,406 deaths; 14,986 hospitalizations; 6,494 blood clots and strokes; 1,598 heart attacks; and 511 miscarriages.” There is an implication that the deaths, hospitalizations, etc. were caused by the vaccine. As I understand it, these totals include statistics for cases which were not caused by the vaccines, but just occurred after the vaccine was given. I may have heard wrong but It’s my understanding that the CDC has not found a case where a death was definitely caused by the vaccine. |
|
|
|
Post by duwayne on Jun 1, 2021 20:49:23 GMT
Missouriboy, you asked, so I’ll give my comments and am eager to hear your (and others) reaction. There is one chart that can be very misleading to the average viewer. It shows a summary of the CDC follow-on report of those who have been vaccinated. "Through May 14, 2021 there have been 227,805 adverse events reported to the CDC from those who received COVID vaccinations. There were 4,201 deaths reported" (which is shown in flaming red). This is enough to cause some to conclude that the vaccine is dangerous. The first question should be, were any of these deaths caused by the vaccine? 158,000,000 people, mostly over 50 have received at least one shot. With that many people, isn’t it logical that some people died? If I heard it correctly, Peter McCullough said a task force from CDC looked into the deaths and of the 1600 that they deemed worthy of analysis, they did not find any they would attribute to the COVID vaccine. He noted the CDC couldn’t have possibly studied the deaths in enough detail to make a firm conclusion. But that is a long way from scientifically proving the COVID vaccines are deadly. My conclusion is the Moderna and Pfizer COVID vaccines are safe. My conclusion also is you are very well protected against COVID 19 and its existing variants either with the COVID vaccine or from having been infected by COVID 19. |
|
|
|
Post by duwayne on May 30, 2021 20:50:44 GMT
www.zerohedge.com/covid-19/ivermectin-new-penicillin"Cases in Delhi, where Ivermectin was begun on April 20, dropped from 28,395 to just 2,260 on May 22. This represents an astounding 92% drop. Likewise, cases in Uttar Pradesh have dropped from 37,944 on April 24 to 5,964 on May 22 - a decline of 84%."
|
|
|
|
Post by duwayne on May 27, 2021 19:45:53 GMT
Is there a link to the Salk study? I didn't see one. I found this recent article which appears to describe the Salk finding you referred to. www.salk.edu/news-release/the-novel-coronavirus-spike-protein-plays-additional-key-role-in-illness/"LA JOLLA—Scientists have known for a while that SARS-CoV-2’s distinctive “spike” proteins help the virus infect its host by latching on to healthy cells. Now, a major new study shows that the virus spike proteins (which behave very differently than those safely encoded by vaccines) also play a key role in the disease itself." Note in the second sentence that this spike protein is not like the vaccine spike protein which they describe as safe. Does anyone have a valid reason for not getting vaccinated other than Ron Paul's reason which is he has already had the virus and is immune and the vaccine should be used by someone who needs it. Being afraid of needles is a pretty weak excuse.  |
|
|
|
Post by duwayne on May 27, 2021 14:03:21 GMT
The Salk researchers are confirming that the main damage from COVID is caused by the spike protein not the virus. And, if that’s the case, then why are we injecting people with vaccines that teach their cells to make spike proteins?Why would we inject climate-cooling materials into an atmosphere that is already cooling? I detect a relative. Is there a link to the Salk study? |
|
|
|
Post by duwayne on May 27, 2021 1:59:08 GMT
I'm too impatient to wait on evolution. Rabies is still with us and I believe it is 100% lethal without medical intervention. There’s smallpox and polio which have not become gentle through evolution. I remember stories about the Aztec population declining from 20 million to 1 million over a 60-year period largely because of disease brought by the Spaniards. Even with that many cases and that many deaths and likely a large number of variants, some of which supposedly increased the deaths, the benign variants did not win out in a timely manner. You have to compare like with like A respiratory RNA virus is not like Smallpox or syphilis. The single RNA molecule has no redundancy and will have a lot of mutations most disbenefit the virus but some may be a benefit. The turn over of infection/contagion in the population is high rather than the slower rate of infection in other diseases. Rabies is not transferrable human to human (to my knowledge) as it is a bacterial infection. Smallpox was infectious for a period when the sufferer was barely symptomatic, polio is not a one and done either: "Most people who get infected with poliovirus (about 72 out of 100) will not have any visible symptoms. {sounds familiar already)
About 1 out of 4 people with poliovirus infection will have flu-like symptoms that may include:
Sore throat
Fever
Tiredness
Nausea
Headache
Stomach pain
These symptoms usually last 2 to 5 days, then go away on their own.
A smaller proportion of people with poliovirus infection will develop other, more serious symptoms that affect the brain and spinal cord:
Paresthesia (feeling of pins and needles in the legs)
Meningitis (infection of the covering of the spinal cord and/or brain) occurs in about 1 out of 25 people with poliovirus infection
Paralysis (can’t move parts of the body) or weakness in the arms, legs, or both, occurs in about 1 out of 200 people with poliovirus infection" www.cdc.gov/polio/what-is-polio/index.htmFrom CDC so it must be right  So Polio may have become less effective at paralyzing sufferers 1 in 200 is a pretty low proportion paralyzed. Also note the similarity of a mild almost asymptomatic disease for most so perhaps a LOT more people are or have had been infected with polio. As with COVID-19 the denominator is a guess so it is not possible to know whether the disease is more or less contagious and thus the real IFR is also a guess. If you add in political and financial imperatives to scare the population the guessing will all be toward an IFR that is high. SARS-CoV-1 had an IFR of around 10%. FauXi must have been REALLY gutted when he realized that all the passaging *GOF had reduced the IFR to a tenth of that or less. Seems that the death rate is hardly different to the expected life expectancy death rates in the population. Nautonnier, this discussion started with your statement. “The evolution pattern of viruses and bacteria - always follows the same path. The high IFR strains kill their hosts too fast and die out…” Given enough time (centuries?) that may be true, I don’t know. I provided a broad range of examples of viruses and bacteria which resulted in massive numbers of deaths over long periods of time. Rabies, even with a death rate of around 100% in its animal hosts has not died out. We’ve seen new strains of COVID which are more contagious and are causing higher rates of infection. There is a possibility of new mutations which are more lethal. The longer COVID hangs around, the greater the possibility of a really bad strain. That’s the science as I see it. |
|
|
|
Post by duwayne on May 26, 2021 16:53:10 GMT
I’m not sure that the natural selection process will necessarily weed out highly lethal viruses. I think the specifics of the virus would be all-important. If the virus is lethal to the point that people immediately die when they are infected, then the virus would die out because there are no spreaders. If people get the virus and go through 2-3 weeks of incubation and spreading and then either recover or die, whether they recover or die wouldn’t matter much with respect to the virus spread. I think COVID is more like the second example. The problem is that there is not that equivalence. The severe cases tend to be hospitalized and taken out of the 'spreader' community faster than the less severe - so the severe virus will not have the same 'spreading' opportunities. Similarly, the less severe strains may be close to asymptomatic so may be spread further and faster particularly if as claimed they are more contagious. It is obviously a 'venn diagram' with some overlap; but overall the less lethal strain will have an evolutionary advantage and become the dominant strain. I'm too impatient to wait on evolution. Rabies is still with us and I believe it is 100% lethal without medical intervention. There’s smallpox and polio which have not become gentle through evolution. I remember stories about the Aztec population declining from 20 million to 1 million over a 60-year period largely because of disease brought by the Spaniards. Even with that many cases and that many deaths and likely a large number of variants, some of which supposedly increased the deaths, the benign variants did not win out in a timely manner. |
|
|
|
Post by duwayne on May 25, 2021 0:15:30 GMT
The Hodcroft charts show how fast a new, more contagious variant can spread, even in a situation where there is a lot of social distancing and vaccinations and immunity. As long as COVID is around, new variants will be generated. A new, highly lethal, highly contagious variant is a possibility. Of course it is possible but it will ( by definition - highly lethal) die out quickly as it is not around long enough to spread to all susceptible hosts as it has killed the hosts that it infected. Survival of the fittest: an equally contagious but less lethal variant will become dominant. Eventually, a symbiosis is achieved where the variant does not kill or even disable the host it may even add some evolutionary advantage and the virus become a part of the DNA of the host That's evolution for you. I’m not sure that the natural selection process will necessarily weed out highly lethal viruses. I think the specifics of the virus would be all-important. If the virus is lethal to the point that people immediately die when they are infected, then the virus would die out because there are no spreaders. If people get the virus and go through 2-3 weeks of incubation and spreading and then either recover or die, whether they recover or die wouldn’t matter much with respect to the virus spread. I think COVID is more like the second example. |
|
|
|
Post by duwayne on May 24, 2021 5:27:37 GMT
The Indian COVID variant now makes up more than 30% of the new cases in the UK where overall reported cases have begun to increase somewhat. The Indian variant is shown in green in the linked charts. covariants.org/per-countryIn the US, the Indian variant makes up only 2% of the cases but its early path doesn't look much different than the UK variant which ultimately dominated in the US. The evolution pattern of viruses and bacteria - always follows the same path. The high IFR strains kill their hosts too fast and die out as SARS1 did, this gives and evolutionary advantage to the low IFR but highly infectious variants which then become dominant. So more people get infected but less have severe disease/hospitalization and death. Politicians cannot grasp this nuance for some reason ( or they want to keep the level of fear as high as possible) So a 'new strain' is treated, as in zombie apocalypse, as a mutant strain that will lead to another wave of deaths: Not true but it serves their political purpose. Scientists like Emma Hodcroft, PhD Institute of Social and Preventive Medicine University of Bern, Switzerland & SIB Swiss Insitute of Bioinformatics, Switzerland; then generate the charts at covariants.org/per-country and the politicians get to say what they 'like' - this does not make the charts wrong it does change them to the propaganda that the politicians want and separates the politicians from the actual charts - so they can rightly say - " not me I couldn't generate a chart like that; this was done for us by an expert in Bioinformatics from the University of Bern" The Hodcroft charts show how fast a new, more contagious variant can spread, even in a situation where there is a lot of social distancing and vaccinations and immunity. As long as COVID is around, new variants will be generated. A new, highly lethal, highly contagious variant is a possibility. |
|
|
|
Post by duwayne on May 23, 2021 14:17:23 GMT
The Australian Bureau of Meteorology is looking for Cycle 25 to be similar to Cycle 24. 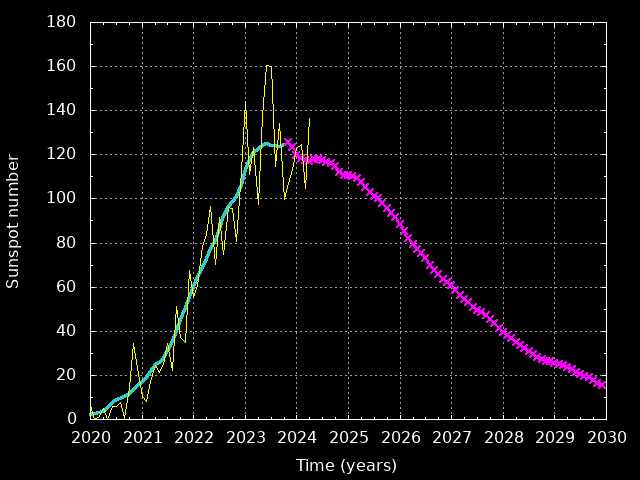 |
|
|
|
Post by duwayne on May 23, 2021 14:02:07 GMT
The Indian COVID variant now makes up more than 30% of the new cases in the UK where overall reported cases have begun to increase somewhat. The Indian variant is shown in green in the linked charts. covariants.org/per-countryIn the US, the Indian variant makes up only 2% of the cases but its early path doesn't look much different than the UK variant which ultimately dominated in the US. |
|
|
|
Post by duwayne on May 20, 2021 16:43:06 GMT
|
|
|
|
Post by duwayne on May 20, 2021 16:34:58 GMT
|
|
|
|
Post by duwayne on May 11, 2021 1:08:29 GMT
While some may be giving up on the AMO as a "stand-alone" climate oscillation, it may yet be found to be tied to other oscillations. This chart is a bit messy, but it seems to show a dramatic temperatue "upshift" of about 1C in Jan-Apr. CET temperatures about 1986 ... coinciding with the start of solar cycle 22 and the mid-point of the AMO shift that started during the last solar minimum in the 1970s. One will remember that the Great Pacific Climate Shift occurred in 1976, just at the large increase from SC20 to SC21. The AMO shifted direction at just that time. Coincidence? This 1C higher Jan-April CET temperature plateau has been very consistent over the last 30 years. But note that CET April, 2021 temperature deviations dropped to the lowest levels since 1986. At the start of new solar cycle 25. Can we now expect the AMO to start its downward trend? Ever wonder how fast temperatures can change? Just look at that 1986-1990 shift. 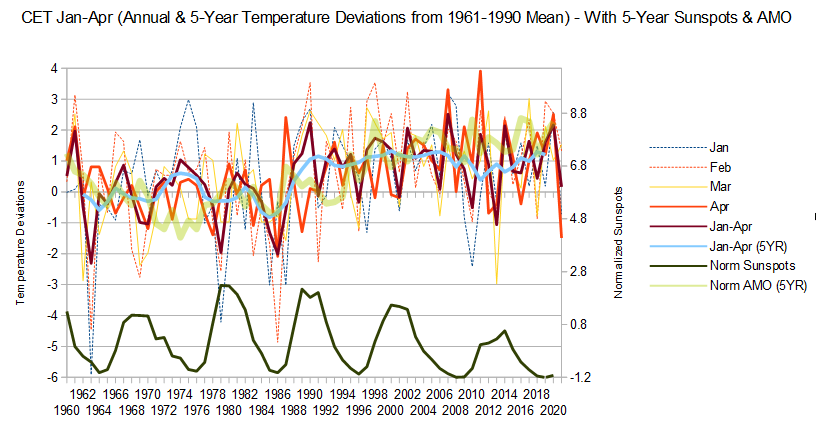 I've always referred to the 60-year Ocean Current Cycle. The AMO is a key part but so far this down cycle its not carrying its share of the load while other oscillators are aiding the cooling. Based on history the AMO should go negative in the future. The warmists will regret any claims that the AMO (and 60 year cycle) isn't real. When temperatures stay low over the next several years, they will need an excuse. I made a prediction here several years ago that the warmists would someday after temperatures don't go up as predicted,jump on the 60-year cycle concept and claim that when the upswing begins things will get really bad. They, of course will overstate the warming by a factor of 2 to 4 as they always do. |
|
|
|
Post by duwayne on May 9, 2021 17:59:26 GMT
I look at other sources of 'infection fear' and the films and videos like "mutant strain" or "Zombie Apocalypse" that really follow the same plot - it is a kind of 'race subconscious'. Along comes a slightly different variant of SARS-CoV-2 and the 'media studies grads' in big tech rush out the same plot that we are all going to die. Except that the way these things work is those strains with the highest IFR die out quickest (by definition). Those variants that have a high infection rate and low fatality rate become the dominant strain - that is the way evolution works. Kill the host organism fast and the variant dies with the hosts. Keep the host organism alive but infectious and the variant becomes dominant but less deadly. Clearly, the variants with the high infection rates become dominant. The daily COVID deaths in India with the new variants are up 4,000% from the level just 2 months ago and still climbing. The new variants do not appear to have a low fatality rate. |
|







